What Is The Hyoid Bone?
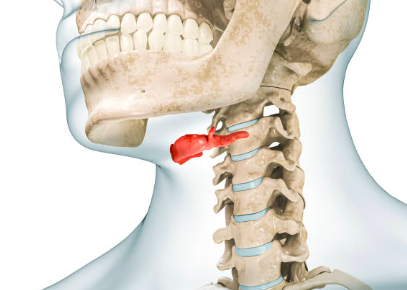
The hyoid bone is a horseshoe shaped bone that sits at the front of the neck (above the thyroid cartilage). It is an anchor point for many of the muscles of the tongue and throat. Although it doesn’t get much attention, it is an important structure for swallowing, speech, chewing and breathing.
Did you know the hyoid bone is the only bone in the body not directly connected to another bone?
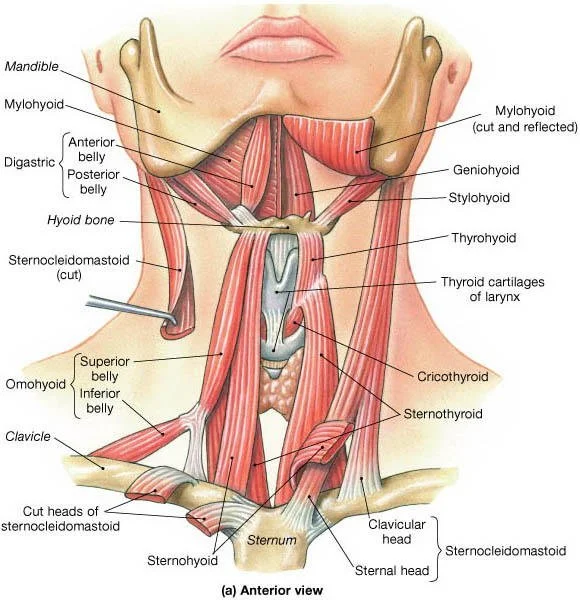
Despite it’s lack of connection to other bones, the hyoid bone is connected to many structures. It serves as an attachment point for:
- the tongue muscles
- the larynx
- the epiglottis
- the pharynx
- the skull
Just like when there is muscle tightness and imbalance in other areas of the body, dysfunction of the muscles in this region can lead to functional issues.
What can happen if there is abnormal movement of the hyoid bone?
Clinical dysfunction of the hyoid bone is known as Hyoid Bone Syndrome. This is typically classified as pain over the muscles and ligaments attached to the hyoid bone due to inflammation and/or degeneration. This can be particularly painful with neck movements and swallowing. Hyoid Bone Syndrome can arise due to past trauma, overuse or degeneration of part of the hyoid bone where the stylohyoid ligament attaches. The pain is typically over the throat region but can radiate to the jaw and is therefore sometimes misdiagnosed as a TMD (TMJ/jaw disorder).
In the absence of acute trauma, hyoid dysfunction can occur from muscle imbalance and tension on the hyoid bone. When muscles attached to the hyoid bone become tight, it can present primarily as reduced tongue function, or altered swallowing and/or breathing.
Several studies have implicated forward head posture and hyoid position in influencing hyoid dysfunction. One study (in patients who wore dentures) found that the hyoid position was influenced by changes in mandibular (lower jaw) position and changes in head and neck posture (4). The position of the lower jaw (mandible) impacts the hyoid position and therefore pharyngeal airway size. The more recessed the mandible (as seen in underdevelopment of the jaw or a class II skeletal pattern), the shorter the pharyngeal airway. The position of the hyoid bone influences the size of the pharyngeal airway and generally, the lower the hyoid position, the smaller the airway. This can contribute to breathing issues like sleep apnoea, as upper airway anatomy plays a large role in obstructive sleep apnoea (OSA). Obesity is also a factor in OSA where it can increase the size of the posterior tongue, displacing the hyoid bone lower and negatively impacting the airway (2).
In a patient with a condition involving over contraction of the neck muscles, Botox was injected as a treatment to relax the muscles. In this case, the neck muscles were weakened so much that the muscles attached to the hyoid bone tightened to compensate for the lack of neck muscle activity. This resulted in impairing the patient’s ability to swallow (1). While this is an extreme case, it demonstrates the importance of the movement of the hyoid bone.
Another study (6) looked at the tone of the muscles connected to the hyoid bone and how it influences the movement of the bone. The study findings suggested that the increased neck muscle tone due to poor posture may encourage a low hyoid position and increase the extent of hyoid bone elevation, increasing the risk of aspiration (inhaling food).
As the hyoid is connected to several structures, dysfunction can lead to an impact on other areas of the body. As the tongue muscles are directly connected to the hyoid, dysfunctional movement can result in a poorly functioning tongue in speaking, chewing and swallowing, with overcompensation of the jaw muscles, possibly leading to jaw pain.
The hyoid bone, while not routinely assessed by healthcare practitioners, is often both directly and indirectly considered by practitioners working in the orofacial field where they may look at swallowing function, jaw function, breathing and posture. Soft tissue therapy and postural and orofacial myofunctional exercises may be given to help forward head posture and muscle function that influence hyoid bone position.
References
1. Chang WK, Kim K, Seo HG, Leigh JH, Bang MS. Posture-Dependent Dysphagia After Botulinum Toxin Type A Injection at Sternocleidomastoid in a Patient With Athetoid Cerebral Palsy. Am J Phys Med Rehabil. 2018 Jun;97(6):e51-e54.
2. Genta PR, Schorr F, Eckert DJ, Gebrim E, Kayamori F, Moriya HT, Malhotra A, Lorenzi-Filho G. Upper airway collapsibility is associated with obesity and hyoid position. Sleep. 2014 Oct 1;37(10):1673-8.
3. Jung-Hsuan Cheng, Szu-Yu Hsiao, Chun-Ming Chen, Kun-Jung Hsu. Relationship between hyoid bone and pharyngeal airway in different skeletal patterns. Journal of Dental Sciences. Volume 15, Issue 3, 2020. Pages 286-293.
4. Tallgren A, Solow B. Long-term changes in hyoid bone position and craniocervical posture in complete denture wearers. Acta Odontol Scand. 1984 Oct;42(5):257-67.
5. Winnberg A, Pancherz H, Westesson PL. Head posture and hyo-mandibular function in man. A synchronized electromyographic and videofluorographic study of the open-close-clench cycle. Am J Orthod Dentofacial Orthop. 1988 Nov;94(5):393-404.
6. Yamazaki Y, Tohara H, Hara K, Nakane A, Wakasugi Y, Yamaguchi K, Minakuchi S. Excessive anterior cervical muscle tone affects hyoid bone kinetics during swallowing in adults. Clin Interv Aging. 2017 Nov 8;12:1903-1910.